Most sourcing problems with 3-ply masks don't start at the factory. They start when a buyer commits to a supplier without understanding which layer drives which test result — and then discovers the problem at customs, or worse, during a hospital procurement audit.
A 3 ply disposable medical mask specification isn't a single number. It's a set of interdependent material and performance parameters, and each one traces back to a specific physical layer. Get the meltblown wrong and your BFE fails. Get the outer spunbond wrong and your fluid resistance rating collapses. Get the ear-loop spec wrong and your product fails a tensile test that most buyers never think to ask about.
This breakdown maps each layer to its function, its material spec, and the test parameter it controls — so you can read a supplier's spec sheet with the same eye we use when we're qualifying our own raw materials.

The SMS Construction: Why Three Layers, Not One
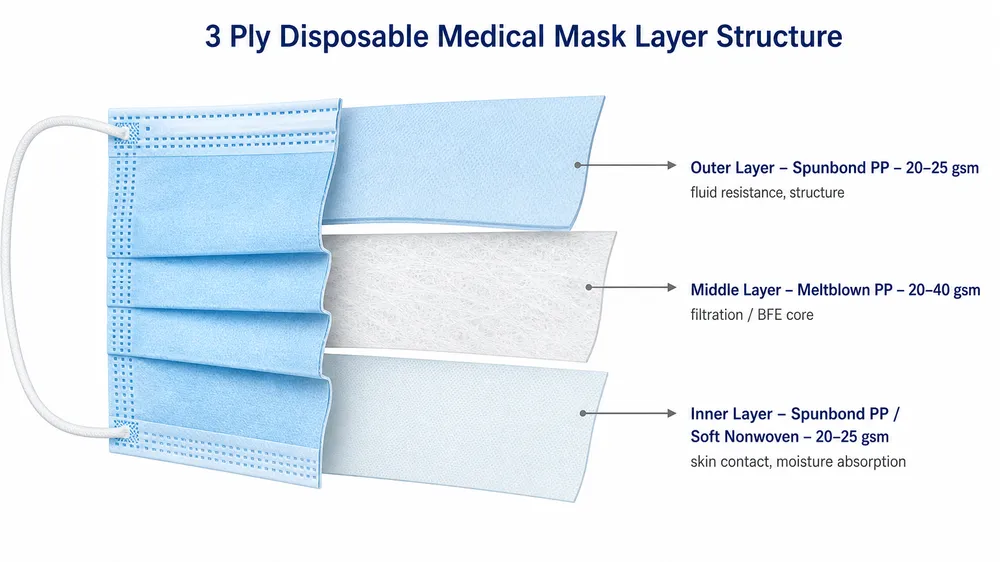
The standard 3-ply disposable medical mask uses an SMS structure — spunbond, meltblown, spunbond. Each layer is a different nonwoven fabric with a different fiber structure, a different basis weight range, and a different job.
The outer spunbond layer faces the environment. The middle meltblown layer does the filtration. The inner spunbond layer sits against the wearer's face. None of these layers is interchangeable, and none of them can compensate for a deficiency in another.
We've seen masks come through our incoming inspection that used a single-layer meltblown construction with a thin spunbond laminate on each side — technically three layers, but not SMS in any meaningful sense. The meltblown was too thin to hold electrostatic charge consistently, and the BFE results were all over the place. The construction looked right on paper. The performance didn't hold.
The table below maps each layer to its material, typical basis weight, primary function, and the test parameter it directly affects.
| Layer | Material | Typical Basis Weight | Primary Function | Test Parameter Affected |
|---|---|---|---|---|
| Outer (Layer 1) | Spunbond PP | 20–25 gsm | Fluid barrier, structural integrity | Fluid resistance (mmHg) |
| Middle (Layer 2) | Meltblown PP | 20–40 gsm | Particulate and bacterial filtration | BFE (%), PFE (%), Delta-P (Pa/cm²) |
| Inner (Layer 3) | Spunbond PP or soft nonwoven | 18–25 gsm | Skin contact, moisture management | Comfort; indirect effect on Delta-P |
The basis weight ranges above are typical for medical-grade product. You'll see cheaper masks using meltblown as light as 15 gsm — that's a cost reduction, not a spec variation. Below roughly 20 gsm, maintaining consistent electrostatic charge across the full roll becomes difficult, and BFE performance starts to drift between batches.
Outer Layer: Fluid Resistance and Structural Integrity
The outer layer is spunbond polypropylene, typically 20–25 gsm. Its job is to resist fluid penetration — blood, respiratory droplets, splash — and to give the mask its structural shape.
The fluid resistance rating on a mask spec sheet (expressed in mmHg) comes from this layer. ASTM F2100 Level 1 requires ≥80 mmHg; Level 2 and Level 3 require ≥120 mmHg and ≥160 mmHg respectively. EN 14683 Type IIR requires ≥120 mmHg splash resistance. A mask that meets Level 1 fluid resistance is not suitable for surgical environments where blood splash is a risk — that's a Level 2 or Level 3 application.
The outer spunbond also affects how the mask holds its shape during wear. A fabric that's too light (below 18 gsm) tends to collapse against the face under normal breathing, which increases Delta-P and makes the mask feel suffocating. We run our outer layer at 20–22 gsm for standard surgical masks — enough structural integrity without adding unnecessary weight to the finished product.
One thing worth checking on any spec sheet: whether the outer layer fabric has been treated for hydrophobicity. Untreated spunbond PP has some natural water resistance, but medical-grade outer layers should carry a hydrophobic finish to meet the fluid resistance thresholds reliably. If a supplier's spec sheet doesn't mention the surface treatment, ask.
Middle Layer: The Filtration Layer That Determines Your BFE and PFE
The meltblown layer is where the actual filtration happens, and it's the layer that most buyers understand least — which is exactly where sourcing risk concentrates.
Meltblown polypropylene is produced by extruding molten PP through fine nozzles under high-velocity hot air, creating a web of extremely fine fibers (typically 1–5 microns in diameter, compared to 15–35 microns for spunbond). The fiber web is then electrostatically charged. That charge is what makes the filtration work: particles are captured not just by mechanical interception but by electrostatic attraction, which is why a 20–25 gsm meltblown layer can achieve ≥95% BFE even though the physical fiber density alone wouldn't block particles that small.
The two variables that determine filtration performance are basis weight and electrostatic charge level. Both need to be controlled consistently across every roll, every batch, every production run.
This is where in-house meltblown production changes the equation. We produce our own meltblown fabric at our Gaomi facility. We set the fiber diameter, the basis weight, and the charge parameters ourselves — and we batch-test every roll before it enters the mask production line. When you order a 3 Ply Disposable Medical Mask from us rated at ≥95% BFE, that number comes from material we made and tested, not from a certificate of conformity from a fabric supplier we're trusting to be consistent.
Factories that buy meltblown from outside suppliers are dependent on that supplier's process consistency. During normal market conditions, that's manageable. During supply disruptions — and we've seen several since 2020 — it's where spec drift happens. A supplier switches to a different meltblown source, the basis weight shifts by 3–5 gsm, the charge retention changes, and the BFE drops from 98% to 91%. The mask looks identical. The test result doesn't.

Inner Layer: Skin Contact and Breathability
The inner layer is spunbond PP or a soft nonwoven blend, typically 18–25 gsm. It doesn't do filtration. Its job is skin contact comfort and moisture management — and it has an indirect effect on Delta-P.
A rough or stiff inner layer increases the perceived resistance to breathing, even if the actual Delta-P measurement is within spec. For hospital and clinical use, where masks are worn for extended shifts, this matters commercially: products that cause discomfort get removed or worn incorrectly, which is a liability issue for the distributor supplying them.
We use a soft-finish spunbond for our inner layer — slightly lower basis weight than the outer layer, with a smoother fiber surface. It's a small material cost difference, but it's the kind of detail that shows up in reorder rates from hospital accounts. (We've had buyers switch to us specifically because their previous supplier's inner layer was causing skin irritation complaints from nursing staff. The filtration spec was fine. The inner layer wasn't.)
The inner layer also affects how the mask sits against the face, which influences the seal quality around the edges. A layer that's too stiff creates gaps at the nose and chin — gaps that bypass the filtration layer entirely. This is a fit issue, not a material spec issue per se, but the inner layer material choice is part of what determines it.
Key Performance Parameters: What the Numbers Mean and Where They Come From
A complete 3 ply disposable medical mask specification includes four performance parameters. Each one maps to a specific test method and a specific layer.
| Parameter | What It Measures | Test Method | Which Layer Drives It |
|---|---|---|---|
| BFE (Bacterial Filtration Efficiency) | % of bacteria-sized particles (3 µm) filtered | ASTM F2101 / EN 14683 Annex B | Meltblown (middle layer) |
| PFE (Particulate Filtration Efficiency) | % of sub-micron particles (0.1 µm) filtered | ASTM F2299 | Meltblown (middle layer) |
| Delta-P (Differential Pressure) | Breathing resistance (Pa/cm²) | ASTM F2101 / EN 14683 Annex C | All three layers combined |
| Fluid Resistance | Resistance to fluid penetration (mmHg) | ASTM F1862 / EN 14683 Annex D | Outer spunbond (layer 1) |
BFE and PFE are both filtration efficiency measurements, but they test different particle sizes. BFE uses a 3-micron aerosol (roughly the size of bacteria-carrying droplets). PFE uses 0.1-micron latex spheres — closer to the size of viral particles. A mask can have high BFE and lower PFE if the meltblown charge isn't optimized for sub-micron capture. For surgical mask applications, BFE is the primary regulatory threshold. For applications where sub-micron filtration matters, check the PFE number specifically.
Delta-P is the pressure differential across the mask at a fixed airflow rate. Lower is better — it means less breathing resistance. ASTM F2100 sets a maximum of 5.0 mm H₂O/cm² for all three levels. EN 14683 sets a maximum of 40 Pa/cm² for Type I and Type II, and 60 Pa/cm² for Type IIR. A mask that passes BFE but fails Delta-P is not compliant — and this is a failure mode we see more often than buyers expect, usually caused by a meltblown layer that's too dense or an inner layer that's too thick.
For a deeper look at how these tests are actually run and what the results mean for your sourcing decisions, see how BFE and PFE testing works on disposable masks.
ASTM F2100 vs EN 14683: Threshold Comparison for US and EU Markets
If you're sourcing for both the US and EU markets, you're working with two different standards frameworks. They test similar parameters but use different thresholds and different classification systems.
| Parameter | ASTM F2100 Level 1 | ASTM F2100 Level 2 | ASTM F2100 Level 3 | EN 14683 Type I | EN 14683 Type IIR |
|---|---|---|---|---|---|
| BFE | ≥95% | ≥98% | ≥98% | ≥95% | ≥98% |
| PFE (0.1 µm) | ≥95% | ≥98% | ≥98% | Not specified | Not specified |
| Delta-P (mm H₂O/cm²) | ≤5.0 | ≤5.0 | ≤5.0 | ≤40 Pa/cm² | ≤60 Pa/cm² |
| Fluid Resistance | ≥80 mmHg | ≥120 mmHg | ≥160 mmHg | Not required | ≥120 mmHg |
| Flammability | Class 1 | Class 1 | Class 1 | Not specified | Not specified |
A few things worth noting in this table:
EN 14683 does not specify PFE. If your EU buyer asks for PFE data, that's a supplementary requirement — common in hospital procurement specs — not a standard EN 14683 threshold. You can still provide it, but it won't appear on the CE technical file as a mandatory parameter.
EN 14683 Type I has no fluid resistance requirement. Type IIR does (≥120 mmHg). If you're selling into surgical environments in Europe, Type IIR is the relevant classification. Type I is for non-surgical medical use.
ASTM F2100 Level 1 is the minimum for US surgical mask clearance. Most hospital procurement specs in the US require Level 2 or Level 3 for procedural and surgical applications. If your buyer is supplying US hospitals, confirm which level their procurement spec requires before you finalize the order.
Our FDA 510(k) registration and CE (EU MDR) certification cover both frameworks, so the documentation is already in place for either market. The spec we ship to you is the spec that clears customs — we don't produce to a different internal standard and then submit third-party tests separately.

Nose Wire and Ear-Loop Specs: The Components That Fail in the Field
Filtration specs get most of the attention. Nose wire and ear-loop specs cause most of the field complaints.
Nose wire is typically a single or double aluminum wire, 0.45–0.55 mm diameter, embedded in the top edge of the mask by ultrasonic welding. The spec parameters that matter are wire gauge, corrosion resistance, and weld integrity. A nose wire that corrodes in humid storage conditions will stain the mask fabric and trigger rejection at incoming inspection. A nose wire that's welded too close to the edge will tear out under normal adjustment — a failure mode that generates returns and warranty claims.
We run our nose wire at 0.5 mm single-core aluminum with a PE coating. The PE coating prevents corrosion and gives the wire enough surface friction to hold its shape after the wearer adjusts it. We test nose wire pull-out force as part of incoming inspection — the wire should require meaningful force to remove, not slide out with finger pressure.
Ear loops are typically flat elastic, 3–4 mm wide, attached by ultrasonic welding. The critical spec is tensile strength — specifically, the force required to break the ear-loop attachment point. ASTM F2100 doesn't specify a minimum ear-loop tensile strength, but hospital procurement specs commonly require ≥10 N at the weld point. We test to ≥15 N as our internal standard, which gives margin above the typical procurement threshold.
Ear-loop material matters too. Cheap elastic loses tension after 2–3 hours of wear, which means the mask starts to sag and the seal degrades. We use a spandex-core flat elastic that maintains tension through a full 8-hour shift. It costs slightly more than standard polyester elastic, but it's the difference between a mask that works for a full clinical shift and one that needs to be replaced at lunch.
(One thing we check at incoming inspection that most buyers never ask about: ear-loop color consistency. If you're running a private-label program with white masks and white ear loops, a batch of slightly off-white elastic is a cosmetic rejection that your end customer will notice. We match ear-loop color to the mask body on every order.)
What a Complete Spec Sheet Should Include for Import and Procurement Audits
A spec sheet that passes a hospital procurement audit or an FDA import review contains more than BFE and PFE numbers. Here's what a complete 3 ply disposable medical mask specification document should include:
Product identification
- Product name and model number
- Applicable standard (ASTM F2100 Level X or EN 14683 Type X)
- Intended use statement
Material specification
- Outer layer: material type, basis weight (gsm), surface treatment
- Middle layer: material type, basis weight (gsm), electrostatic charge method
- Inner layer: material type, basis weight (gsm)
- Nose wire: material, gauge, coating
- Ear loop: material, width, attachment method
Performance test results (with test report reference numbers)
- BFE (%) — test method and result
- PFE (%) — test method and result (if required)
- Delta-P (Pa/cm² or mm H₂O/cm²) — test method and result
- Fluid resistance (mmHg) — test method and result (if applicable)
- Flammability class (if ASTM F2100)
Regulatory documentation
- ISO 13485 certificate number and scope
- CE certificate number (for EU market)
- FDA 510(k) number (for US market)
- Third-party test lab name and accreditation
Traceability
- Batch/lot number system
- Production date range
- Shelf life and storage conditions
If a supplier's spec sheet is missing the material specification section — particularly the meltblown basis weight and the third-party test lab reference — that's a gap worth asking about before you place an order. A spec sheet that only lists performance results without identifying the materials that produce them gives you no way to verify consistency across batches.
Our spec sheets include all of the above. The test reports that travel with each shipment reference the specific production batch, the in-house test results, and the third-party lab verification. That documentation is what your customs broker and your buyer's compliance team will ask for.
How to Verify Spec Claims Before You Commit
Reading a spec sheet is the first step. Verifying it is the second — and most buyers skip it.
Request the third-party test report, not just the certificate. A certificate of conformity says the product meets a standard. The test report shows the actual measured values. BFE of 98.7% is more useful than "meets ASTM F2100 Level 2" because it tells you how much margin exists above the threshold. A product that tests at 98.1% and a product that tests at 99.4% both "meet Level 2," but they're not the same product.
Check the test lab accreditation. The test report should come from an ISO 17025-accredited laboratory. For US market products, Nelson Labs and SGS are commonly recognized. For EU market products, look for a notified body-accredited lab. An in-house test report without third-party verification is not sufficient for import documentation.
Ask about batch-to-batch consistency, not just the certification sample. Certification testing is typically done on a single production sample. What you need to know is whether the factory tests every production batch — or only the batch that went to the certification lab. Under ISO 13485, every batch should be tested before shipment. If a supplier can't tell you their batch testing protocol, that's a sourcing risk.
Request a sample before committing to volume. This sounds obvious, but a surprising number of buyers skip it on repeat orders from the same supplier, assuming the spec hasn't changed. We recommend requesting a sample from any new production run if the order is going into a regulated procurement channel. The sample costs almost nothing. A non-compliant shipment costs significantly more.
We test every production batch in our in-house QC lab — BFE, PFE, and Delta-P — before the batch moves to outgoing inspection. Third-party test reports are submitted for certification documentation. The in-house testing is what catches problems before they become your problem.
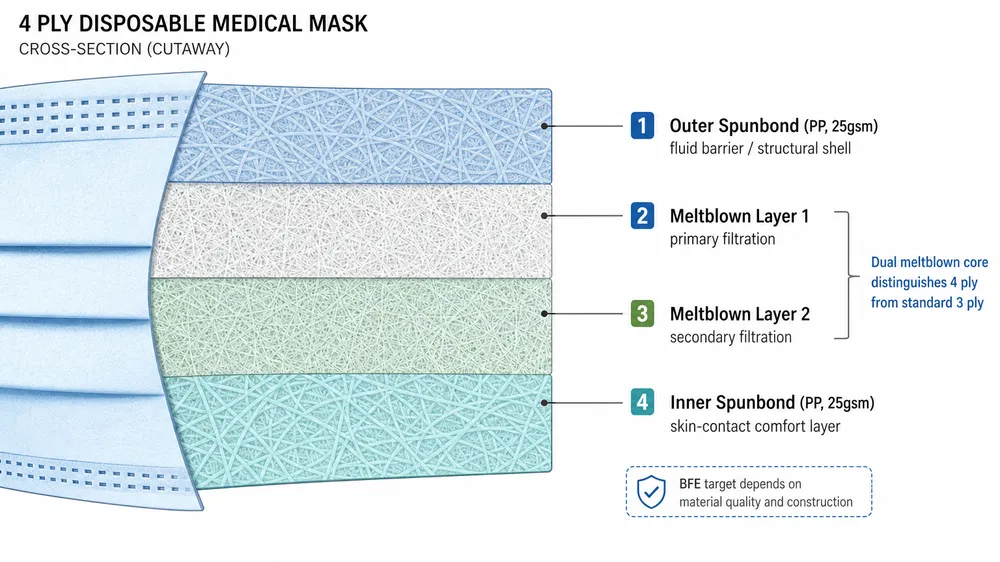
For buyers comparing 3-ply and 4-ply configurations, the layer structure and spec implications are different enough to warrant a separate look — see our breakdown of 3 ply vs 4 ply disposable medical mask differences.
Frequently Asked Questions
What is the difference between BFE and PFE in a 3 ply mask spec?
BFE (Bacterial Filtration Efficiency) measures how well the mask filters bacteria-sized particles at 3 microns, using a standardized aerosol challenge. PFE (Particulate Filtration Efficiency) tests sub-micron particles at 0.1 microns — closer to the size of viral aerosols. Both are driven by the meltblown middle layer. ASTM F2100 requires both; EN 14683 only specifies BFE. If your buyer's procurement spec asks for PFE data on an EN 14683 product, that's a supplementary requirement you need to confirm with your supplier separately.
Can a 3 ply mask meet both ASTM F2100 and EN 14683 simultaneously?
Yes, with the right spec. A mask built to ASTM F2100 Level 2 (≥98% BFE, ≥120 mmHg fluid resistance, ≤5.0 mm H₂O/cm² Delta-P) will generally satisfy EN 14683 Type IIR thresholds as well, since the ASTM Level 2 fluid resistance requirement (≥120 mmHg) matches the Type IIR requirement. The main gap is flammability — ASTM F2100 requires Class 1 flammability testing, which EN 14683 does not specify. A dual-market product needs both test reports in the documentation package.
Why does meltblown basis weight matter for spec consistency across batches?
Meltblown filtration performance depends on both fiber density (basis weight) and electrostatic charge. If the basis weight varies between rolls — say, from 22 gsm to 18 gsm — the charge retention changes, and BFE can drop by several percentage points even if the production process looks identical. This is why in-house meltblown production matters: the factory controls the variable that determines filtration performance, rather than accepting whatever the fabric supplier ships. Batch-to-batch BFE variation of more than 1–2% on a well-controlled production line is a signal worth investigating.
What should I ask a supplier if their spec sheet only shows BFE and PFE numbers?
Ask for the third-party test report (not just the certificate), the meltblown basis weight and material source, the batch testing protocol under their QMS, and the specific ASTM or EN standard level the product is certified to. A spec sheet that lists performance numbers without identifying the materials and test methods behind them gives you no way to verify consistency. If the supplier can't provide the test report with the lab accreditation number, that's a documentation gap that will surface during import review or procurement audit.
What is the minimum ear-loop tensile strength for hospital procurement?
ASTM F2100 doesn't specify a minimum ear-loop tensile strength, but hospital and institutional procurement specs commonly require ≥10 N at the weld point. Our internal standard is ≥15 N, tested at incoming inspection on every ear-loop lot. If you're supplying into a hospital tender, ask your buyer's procurement team for their specific tensile requirement — it varies by institution and country.
If you're ready to evaluate a specific spec configuration — ASTM F2100 Level 1, 2, or 3, or EN 14683 Type I or IIR — send your target standard, required BFE grade, order volume, and any packaging requirements to Request Quote. We'll respond with a spec sheet, third-party test report references, and sample availability.
For the full product range and standard SKU configurations, see our Disposable Medical Masks category page.