Most buyers who've had a shipment fail BFE testing didn't get unlucky. They sourced from a factory that was cutting corners on the meltblown layer — and had no way to know it until the test report came back.
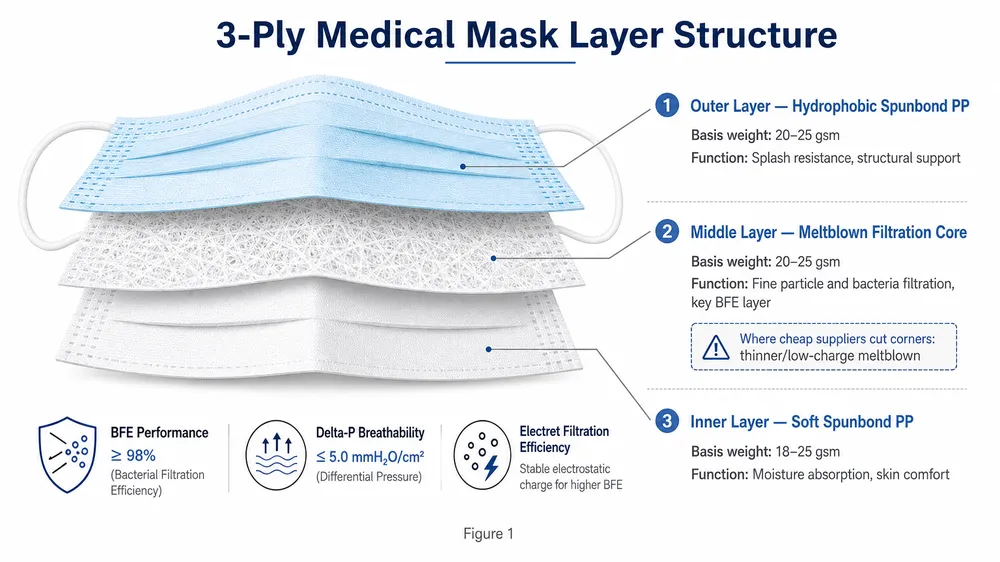
The three-layer structure of a standard 3 Ply Medical Mask looks simple on paper: outer spunbond, meltblown filtration core, inner spunbond. But the performance gap between a mask that passes ≥95% BFE and one that fails isn't random. It's the direct result of specific material choices — basis weight, fiber diameter, electrostatic charge — that are invisible to the eye and easy to fake on a spec sheet.
This article breaks down what each layer actually does, what the performance-critical parameters are, and where the shortcuts happen. If you're sourcing 3-ply surgical masks for distribution, hospital supply, or private-label programs, this is the technical foundation you need before you evaluate a supplier.

Layer 1 — outer spunbond: fluid barrier and structural shell
The outer layer is polypropylene (PP) spunbond nonwoven, typically running between 20–25 g/m² basis weight. Its job is two things: block fluid splash and give the mask its structural shape.
The hydrophobic treatment applied to this layer is what makes it repel blood, saliva, and respiratory droplets rather than absorbing them. Under ASTM F2100 and EN 14683, fluid resistance is a rated performance parameter — Level 1 masks require resistance to 80 mmHg synthetic blood splash, Level 2 and Level 3 step up from there. The outer spunbond is the layer that carries that rating.
Where suppliers cut corners here: underweight fabric. A 20 g/m² outer layer is the standard minimum for a mask that holds its shape and maintains fluid resistance. Some factories drop to 17–18 g/m² to reduce material cost. The mask looks identical. The fluid resistance degrades, and the structural integrity under extended wear weakens. You won't see it in a visual inspection — you'll see it in a fluid resistance test or in field complaints from end users.
The other shortcut is skipping or reducing the hydrophobic treatment. Untreated or undertreated spunbond absorbs moisture instead of repelling it. The outer layer becomes a wick rather than a barrier. This is particularly relevant for buyers supplying clinical environments where splash exposure is a real risk.
What to request: ask for the outer layer basis weight (g/m²) and the hydrophobic treatment specification. A supplier who can't provide these numbers is either buying fabric without spec documentation or doesn't want you to know what's in the mask.
Layer 2 — meltblown filtration core: the layer that determines whether your mask passes or fails
This is the one that matters most. The meltblown layer is the reason a 3-ply surgical mask filters bacteria and particles — and it's the layer where the widest quality gap exists between compliant manufacturers and cheap suppliers.
Meltblown nonwoven is produced by extruding polypropylene through extremely fine nozzles under high-velocity hot air, creating fibers in the 1–5 micron diameter range. The resulting fabric has a dense, random fiber matrix that physically traps particles. But physical filtration alone isn't enough to reach ≥95% BFE. The second mechanism is electrostatic charge — the meltblown fabric is corona-charged during production, creating an electrostatic field that attracts and holds charged particles and aerosols that would otherwise pass through the fiber matrix.
A properly produced meltblown layer for a ≥95% BFE mask typically runs at 20–25 g/m² basis weight. For ≥98% BFE (required for ASTM F2100 Level 2 and Level 3), the basis weight is higher — typically 25–30 g/m² — and the electrostatic charge level is more tightly controlled.

The two shortcuts that cause BFE failures:
Reduced basis weight. Dropping the meltblown from 22 g/m² to 15 g/m² cuts material cost significantly. The mask still has three layers. It still looks like a surgical mask. But the fiber density is too low to reliably achieve ≥95% BFE, and the results become inconsistent — some batches pass, some don't, depending on production variables that day.
Missing or degraded electrostatic charge. Meltblown fabric loses its electrostatic charge over time, especially when stored improperly (high humidity, UV exposure, contact with certain chemicals). Some factories use meltblown that was never properly charged to begin with, or use fabric that has been sitting in a warehouse long enough that the charge has dissipated. A mask made with uncharged meltblown at standard basis weight will typically test in the 60–75% BFE range — well below the ≥95% threshold. The fiber matrix is intact; the electrostatic mechanism is gone.
We produce our meltblown in-house. That's not a marketing point — it's the operational reason we can guarantee spec consistency across large orders. When you buy meltblown from a third-party fabric supplier, you're trusting their production parameters, their storage conditions, and their batch-to-batch consistency. We set the fiber diameter, the basis weight, and the charge level ourselves, and we batch-test every roll before it goes into production. (We've seen what happens when factories don't do this. During the 2020–2021 supply crunch, meltblown from some spot-market suppliers was arriving with BFE performance in the 50–60% range. Factories that didn't have in-house testing capability were shipping non-compliant product without knowing it.)
For more on how meltblown quality connects to BFE outcomes, see our detailed guide on meltblown quality in surgical masks.
Layer 3 — inner spunbond: breathability and Delta-P compliance
The inner layer — the one that sits against the face — is also PP spunbond, but typically softer and lighter than the outer layer, running 18–20 g/m². Its primary function is comfort and breathability, but it has a direct effect on a performance parameter that buyers often overlook: Delta-P, the pressure differential across the mask.
Delta-P measures airflow resistance. Under ASTM F2100, the maximum allowable Delta-P is 5.0 mm H₂O/cm² for Level 1 and Level 2 masks, and 5.0 mm H₂O/cm² for Level 3 as well. EN 14683 uses a similar threshold. A mask that exceeds the Delta-P limit is technically non-compliant — it's too restrictive to breathe through comfortably, which matters for extended clinical wear.
The inner spunbond contributes to Delta-P because it adds airflow resistance on top of the meltblown layer. If a supplier substitutes a denser or heavier inner layer — either to reduce cost on the outer layer and compensate structurally, or simply because they're buying whatever nonwoven is available — the combined Delta-P of the three layers can push the mask over the compliance threshold.
The other substitution we see: replacing the soft inner spunbond with a rougher, cheaper nonwoven grade. This doesn't affect BFE directly, but it affects end-user compliance. Masks that are uncomfortable to wear get pulled down or removed, which eliminates whatever protection they provide. For buyers supplying hospital or institutional channels, this is a downstream liability issue — your customer's procurement team will notice the complaint rate.
| Layer | Material | Typical Basis Weight | Primary Function | Key Performance Parameter |
|---|---|---|---|---|
| Outer | PP Spunbond (hydrophobic) | 20–25 g/m² | Fluid barrier, structural shell | Fluid resistance (ASTM F2100) |
| Middle | PP Meltblown | 20–30 g/m² | Particle/bacterial filtration | BFE ≥95% or ≥98%, PFE |
| Inner | PP Spunbond (soft) | 18–20 g/m² | Comfort, breathability | Delta-P ≤5.0 mm H₂O/cm² |
Where cheap suppliers cut corners: the failure modes in practice
The shortcuts above don't happen in isolation. A factory optimizing for the lowest possible unit cost typically cuts across all three layers simultaneously. Here's what that looks like in practice:
Single-layer substitution. Some factories produce what they call a "3-ply" mask using two layers of spunbond and a thin layer of tissue paper or low-grade nonwoven in place of meltblown. The mask has three layers. It has no filtration capability. BFE testing will return results in the 30–50% range. This is the most egregious version of the shortcut, and it's more common than buyers expect — particularly in very low price-point sourcing.
Reduced meltblown GSM with no disclosure. The factory uses genuine meltblown but at 12–15 g/m² instead of the 20–25 g/m² required for reliable ≥95% BFE. The spec sheet says "meltblown middle layer." It doesn't say the basis weight. The mask may pass BFE testing on a good production day and fail on a bad one, creating inconsistent batch results that are difficult to trace.
Uncharged or degraded meltblown. As described above — the fiber matrix is present, the electrostatic mechanism is absent. BFE results cluster in the 60–75% range. The factory may not even know this is happening if they're not running in-house BFE testing on each batch.
Non-cleanroom production. A mask produced outside a controlled environment can have particulate contamination embedded in the nonwoven layers. For buyers supplying hospital procurement channels, this is a compliance issue — hospital procurement standards typically require cleanroom manufacturing documentation. A factory that can't provide ISO 8 or equivalent cleanroom certification is producing in an uncontrolled environment.
Ear-loop and nose wire shortcuts. These don't affect BFE directly, but they affect the mask's ability to seal properly. An ear loop with insufficient tensile strength breaks under normal use. A nose wire that doesn't hold its shape leaves gaps at the nose bridge. Both reduce effective filtration regardless of what the meltblown layer is rated at.

How to verify layer integrity before accepting a shipment
The documents that matter — and the questions that reveal whether a supplier actually has them.
BFE test report. This is the non-negotiable baseline. The report should show the BFE percentage, the test method (ASTM F2100, EN 14683, or equivalent), the testing laboratory, and the lot or batch number. A test report without a batch number is a generic certificate — it tells you a mask from that factory passed BFE testing at some point, not that your specific shipment will.
Material specification sheet. Request the spec sheet for the meltblown layer specifically: basis weight (g/m²), fiber diameter range, and electrostatic charge specification. If the supplier can't provide this, they're either buying meltblown without spec documentation or they don't want you to know the basis weight. Both are red flags.
Batch traceability documentation. Under ISO 13485, every production batch should be traceable to its raw material lots. Ask for the batch record or material traceability document for your specific order. A factory operating under a real ISO 13485 QMS can produce this. A factory with a decorative certificate cannot.
Cleanroom certification. For hospital or institutional supply channels, ask for the cleanroom classification certificate and the most recent environmental monitoring report. ISO 8 (Class 100,000) is the standard for medical mask production. If the factory can't provide this, the production environment is uncontrolled.
Delta-P test result. Often overlooked, but required for ASTM F2100 compliance. The Delta-P result should be in the same test report as BFE, or in a separate breathability test report. A mask that passes BFE but fails Delta-P is non-compliant.
The question that separates real manufacturers from trading companies: "Can you provide the meltblown basis weight specification and the in-house BFE test data for the last three production batches?" A factory with in-house testing capability and in-house meltblown production can answer this immediately. A factory buying meltblown from outside and relying on third-party testing will either deflect or provide a generic certificate.
For a deeper look at how to interpret BFE and Delta-P test results when evaluating suppliers, see our guide on BFE and Delta-P performance.
What in-house meltblown production means for your order consistency
Batch-to-batch BFE variance is the sourcing problem that doesn't show up until you're three orders in. The first order passes testing. The second order passes. The third order fails — or passes at 95.2% when your customer's procurement spec requires ≥98%. The factory blames the testing lab. You're holding a non-compliant shipment.
This is almost always a meltblown sourcing problem. Factories that buy meltblown from third-party suppliers are dependent on that supplier's production consistency, storage conditions, and honesty about what they're shipping. When the meltblown supplier has a bad production run, or ships older stock with degraded charge, or substitutes a lower basis weight to manage their own costs, the mask factory may not know until the BFE test comes back.
We brought meltblown production in-house specifically to eliminate this variable. Our meltblown line runs to fixed parameters: fiber diameter, basis weight, and charge level are set for each filtration target and verified on every roll before it enters the mask production line. When you order a ≥95% BFE mask from us, the meltblown going into that mask was produced in our facility, tested in our lab, and meets the spec we committed to. When you order ≥98% BFE, the parameters are adjusted accordingly — we're not hoping the fabric supplier shipped the right grade.
Our in-house QC lab runs BFE, PFE, and Delta-P testing on every production batch. The test data is available per batch, not just per product line. If you're building a private-label program or supplying a hospital procurement channel that requires per-lot test documentation, we can provide it — because we generate it as part of standard production, not as a special request.
The certification stack — ISO 13485:2016, CE under EU MDR, FDA 510(k) registration — means the layer specifications and QC procedures are documented under a regulated quality management system. The meltblown basis weight, the charge specification, the BFE acceptance criteria — these are controlled documents, not informal practices. When your compliance team or your customer's procurement auditor asks for the technical file, it exists.
Our Surgical Medical Masks product range covers standard 3-ply configurations at both ≥95% and ≥98% BFE grades, with full test documentation available for each SKU.
Sourcing decision guide: what to specify and what to verify
If you're evaluating 3-ply surgical mask suppliers, here's the practical framework:
Specify by performance grade, not just "3-ply surgical mask." The difference between a ≥95% BFE mask and a ≥98% BFE mask is a different meltblown spec. Tell your supplier which grade you need and ask for the test report that confirms it. If they can't distinguish between the two, they're not controlling the meltblown layer.
Request per-batch test reports, not just product certificates. A product certificate tells you the design was tested. A per-batch report tells you your specific shipment was tested. For large orders or ongoing supply programs, per-batch documentation is the only way to catch batch-to-batch variance before it becomes a compliance problem.
Ask about meltblown sourcing before you ask about price. "Do you produce meltblown in-house or purchase from a third-party supplier?" is the single most useful question you can ask a mask supplier. The answer tells you how much control they have over the variable that determines BFE performance. A factory that buys meltblown from outside can still produce compliant masks — but their consistency depends on their supplier's consistency, and that's a risk you're carrying.
Verify cleanroom status if your channel requires it. Hospital procurement, government tenders, and institutional supply chains increasingly require cleanroom manufacturing documentation. Get the certificate before you commit to the order, not after.
Sample before scaling. For new supplier relationships, a sample order with independent BFE testing is the lowest-cost way to verify what you're actually getting. Send samples to an accredited third-party lab — Nelson Labs, SGS, Intertek — and compare the results against the supplier's own test report. If the numbers diverge significantly, you have your answer.
The masks that fail in the field — the ones that generate complaints, failed audits, or customs holds — almost always trace back to a meltblown layer that wasn't what the supplier claimed. The layer structure of a 3-ply mask is simple. The quality controls required to make it perform consistently are not.
If you're ready to specify your BFE grade and order volume, Request Quote and we'll respond with the relevant spec sheet, per-batch test report references, and a production timeline for your destination market.
Frequently asked questions
What is the minimum meltblown basis weight for a ≥95% BFE 3-ply surgical mask?
The typical minimum is around 20 g/m², but basis weight alone doesn't guarantee BFE performance — the electrostatic charge level is equally important. A meltblown layer at 20 g/m² with proper corona charging will typically achieve ≥95% BFE. The same basis weight with degraded or absent charge may test in the 60–75% range. When evaluating suppliers, ask for both the basis weight specification and confirmation that the fabric is corona-charged during production.
Can I verify meltblown quality from a finished mask sample?
Not visually. The only reliable verification method is BFE testing at an accredited lab. You can request the meltblown spec sheet from the supplier and cross-reference it against the BFE test report, but the definitive check is independent testing of your actual sample. Some buyers also request a material cross-section or basis weight measurement from a fabric sample cut from the mask — this confirms the layer weight but not the charge level.
What's the difference between BFE and PFE, and which matters for my sourcing decision?
BFE (Bacterial Filtration Efficiency) measures the mask's ability to filter bacteria-sized particles (typically 3.0 micron challenge aerosol). PFE (Particulate Filtration Efficiency) measures filtration of sub-micron particles (typically 0.1 micron latex spheres). For standard surgical mask applications — clinical environments, general healthcare, institutional supply — BFE ≥95% is the primary compliance threshold. PFE becomes relevant when your buyers are supplying environments with sub-micron aerosol exposure risk, or when the procurement spec explicitly requires it. ASTM F2100 Level 2 and Level 3 require both BFE ≥98% and PFE ≥98%.
Why do some 3-ply masks fail BFE testing even when they have a meltblown layer?
Three common reasons: the meltblown basis weight is too low to achieve consistent filtration, the electrostatic charge has degraded (from improper storage or poor production), or the meltblown was never properly charged to begin with. A fourth reason that's less obvious: the mask construction itself — specifically the edge sealing — can create bypass paths where air flows around the meltblown layer rather than through it. Ultrasonic welding with proper seam geometry eliminates this; adhesive bonding or heat sealing with poor tolerances can leave gaps.
What documents should I request before placing a bulk order?
At minimum: BFE test report with batch number, material specification sheet for the meltblown layer (basis weight and charge spec), ISO 13485 certificate, and cleanroom classification documentation. For US import: FDA 510(k) registration number. For EU import: CE technical file reference and EU MDR declaration of conformity. For hospital or institutional supply: per-lot test reports and batch traceability records. If a supplier can't provide all of these before you place the order, the documentation gap will surface at customs or during your customer's procurement audit.