The Fit Complaint Problem Behind This Decision
The attachment style question surfaces in procurement when fit complaints start accumulating. Staff report ear soreness after six-hour shifts. OR nurses flag that ear-loop masks shift during procedures. Infection control flags inconsistent seal. The product spec looks fine on paper — BFE ≥95%, ASTM Level 2 — but the attachment method is generating friction that shows up as compliance failures, not filtration failures.
Here's the short answer: ear-loop masks are the right default for general clinical and outpatient settings where volume, donning speed, and SKU simplicity matter. Tie-on masks belong in the OR, sterile-field environments, and any setting where staff wear masks for six or more hours continuously and need to adjust fit without breaking protocol.
The rest of this article explains why, and what to verify when you're sourcing either configuration.

Ear Loop vs Tie-On: The Specification Matrix
| Dimension | Ear Loop | Tie-On |
|---|---|---|
| Attachment method | Ultrasonic-welded elastic loop | Fabric or nonwoven tie, knotted at back of head/neck |
| Fit adjustability | Fixed loop length — no field adjustment | Fully adjustable — tied to fit |
| Ear pressure risk | Present on extended wear (6+ hours) | None — no ear contact |
| Donning speed | Fast — 5–10 seconds | Slower — 20–30 seconds, requires two hands |
| Extended-wear suitability | Moderate (up to ~4 hours comfortably) | High — suitable for full surgical shifts |
| Seal consistency | Loop tension varies by face geometry | Tie tension controlled by wearer |
| Bond method (eztio) | Ultrasonic weld — machine-controlled | Ultrasonic weld — same process, same bond strength |
| Standard SKU availability | High — dominates volume orders | Lower — typically requires confirmed volume |
| MOQ (eztio standard) | 50,000 pieces | Confirmed volume required |
| Typical clinical setting | General ward, outpatient, clinic | OR, sterile field, ICU extended wear |

Where Ear Pressure Becomes a Procurement Problem
The ear pressure issue with elastic loops isn't a comfort complaint — it's a compliance signal. When staff start pulling masks down between patient interactions because the loops are cutting into their ears, the mask is no longer doing its job. That's the downstream cost that doesn't show up in the unit price comparison.
We see this pattern most often in two settings: high-volume wards where staff are masked for full 8–12 hour shifts, and emergency departments where the pace makes mask adjustment a constant friction point. In both cases, the fit complaint isn't about filtration performance — BFE and PFE are fine. The attachment method is creating a compliance failure that the filtration spec can't fix.
Elastic loop tension is the variable that determines whether this becomes a problem. Loops that are too tight create pressure; loops that are too loose break the facial seal. The spec we test at incoming inspection is tensile strength — we verify that every lot of elastic meets our minimum pull-force threshold before it enters production. (We've seen incoming elastic that passes visual inspection but fails tensile testing — it looks fine, stretches fine by hand, but fatigues faster than spec under repeated donning cycles. That's why we test it, not just look at it.)
Tie-on masks eliminate this variable entirely. The wearer controls the tension at donning. In OR settings, where the mask goes on once and stays on for the duration of a procedure, that adjustability is the reason tie-on has been the standard for surgical use for decades. The fit is set by the person wearing it, not by a fixed elastic dimension that may or may not match their face geometry.
Application Showdown: Which Style Wins in Your Setting
General Ward and Outpatient: Ear Loop
For general clinical use — outpatient clinics, general wards, administrative areas, pharmacy — ear-loop masks are the right call. Donning speed matters when staff are masking and unmasking dozens of times per shift. The SKU is simpler to manage, MOQ is lower, and the volume economics work in your favor. A 50,000-piece standard ear-loop order ships on a predictable schedule; you're not managing a specialty SKU with longer lead times or uncertain availability.
The fit complaint risk in these settings is manageable because wear duration per session is typically shorter. Staff aren't masked continuously for eight hours — they're masking for patient interactions and removing between. Ear pressure doesn't accumulate the same way it does in OR or ICU environments, so the elastic loop's fixed tension is adequate for the wear pattern.
Winner: Ear loop. Lower unit cost, faster donning, simpler sourcing, adequate fit for intermittent wear.
Operating Room and Sterile Field: Tie-On
The OR is where tie-on masks earn their place. Procedures run two to six hours. The mask goes on before scrubbing and doesn't come off until the procedure ends. Ear loops in this context create two problems: progressive ear pressure that becomes genuinely painful by hour three, and the risk that a staff member adjusts the mask mid-procedure — breaking sterile field protocol to relieve discomfort.
Tie-on masks solve both. The wearer sets the tension at donning, the mask stays put, and there's no ear contact to create pressure. The slower donning time is irrelevant in an OR context where the mask is worn for the duration of a case, not put on and taken off repeatedly.
The other factor: OR procurement typically runs through a different channel than general ward supply. Tie-on masks are often specified by the surgical team or infection control, not selected from a general supply catalog. If you're distributing into hospital systems, carrying both configurations lets you serve both channels without sending buyers elsewhere for the OR SKU.
Winner: Tie-on. Extended wear, sterile-field compliance, no ear pressure accumulation.
ICU and High-Acuity Settings: Tie-On
ICU staff face the same extended-wear problem as OR staff, with the added complexity of frequent patient interaction. Masks stay on for long stretches, but staff are also moving between patients, adjusting PPE, and working in environments where fit integrity matters more than in general wards.
Some facilities use ear-loop masks with ear-saver accessories — a strap that clips behind the head and takes the loop tension off the ears — but that's a workaround, not a solution. It adds a separate accessory to manage, and the clip can interfere with other PPE. If your buyer is stocking ICU supply, tie-on is the cleaner specification.
Winner: Tie-on for full-shift ICU use. Ear loop with ear-saver is a viable compromise if tie-on SKU availability is a constraint, but it introduces an accessory dependency that tie-on eliminates.

What to Verify When Sourcing Either Configuration
The attachment style question is separate from the filtration question, but buyers sometimes conflate them. A few things worth confirming before you commit to a supplier:
Filtration spec is independent of attachment style. BFE and PFE numbers come from the meltblown layer, not the ear loops or ties. A supplier who can only hit BFE ≥95% on their ear-loop SKU but not their tie-on SKU has a production consistency problem — the mask body should be identical regardless of how it attaches. We produce both configurations from the same mask body and the same meltblown layer. The attachment method is the last step in the production process, not a variable that affects what's in the filtration layer. Because we produce our own meltblown fabric in-house, the filtration spec is controlled at the source — we're not dependent on a third-party fabric supplier's batch consistency.
Ask how the attachment is bonded. Ultrasonic welding produces a consistent, machine-controlled bond. Adhesive bonding introduces variability — bond strength depends on adhesive application consistency, temperature, and surface prep. We use ultrasonic welding on both ear-loop and tie-on configurations, so the bond strength is determined by machine parameters, not operator technique. Ask your supplier which method they use and whether they have tensile test data to back it up. This is a spec point that most suppliers don't surface proactively, but it's the difference between a loop that holds through a full shift and one that fails at the weld point.
Verify the elastic spec on ear-loop masks. Elastic that fatigues prematurely is the most common source of ear-loop fit complaints. The loop should maintain consistent tension across the expected wear duration of a single-use mask. We test incoming elastic lots for tensile strength and elongation recovery before they enter production — this is part of our ISO 13485 incoming inspection protocol, not an optional QC step. If a supplier can't tell you what tensile spec their elastic meets or how they verify it at incoming inspection, that's a gap worth probing before you commit to a volume order.
Understand the MOQ structure before you spec the configuration. Standard ear-loop SKUs are high-volume items — our 50,000-piece MOQ reflects that. Tie-on configurations are lower-volume specialty items, and the MOQ structure reflects the line setup and material procurement involved. If you're building a mixed order — ear-loop for general ward, tie-on for OR — confirm the MOQ for each SKU separately and plan your order accordingly. We can consolidate both configurations in a single shipment with separate lot documentation for each SKU.
Sourcing Trade-Offs by Attachment Type
The procurement reality is that ear-loop masks dominate volume orders for a reason. They're faster to produce, easier to stock, and the elastic supply chain is more stable than specialty tie materials. For distributors building a hospital supply catalog, ear-loop is the core SKU and tie-on is the specialty add-on.
That said, the tie-on segment is not a niche. OR supply is a distinct procurement channel with its own specifications, and facilities that run high surgical volumes need a reliable tie-on source. If you're distributing into hospital systems rather than just outpatient or clinic networks, carrying both configurations is the right inventory strategy — the two SKUs serve different buyers within the same institution.
For our Ear Loop Disposable Medical Mask line, standard SKUs are available at 50,000-piece MOQ with 15–25 day lead time from order confirmation. Tie-on configurations are available with confirmed volume — send us your estimated monthly requirement and we'll confirm MOQ and lead time for your specific configuration. Both carry the same certification stack: ISO 13485:2016, CE (EU MDR), FDA 510(k) registered. The filtration spec — BFE ≥95%,tested in-house on every production batch — is identical across attachment styles. You're not trading filtration performance for fit when you move between configurations.
For a full overview of our Disposable Medical Masks product range, including available grades and configurations, see the category page.
FAQ: Attachment Style Selection for Clinical Procurement
Does the attachment style affect the mask's filtration rating?
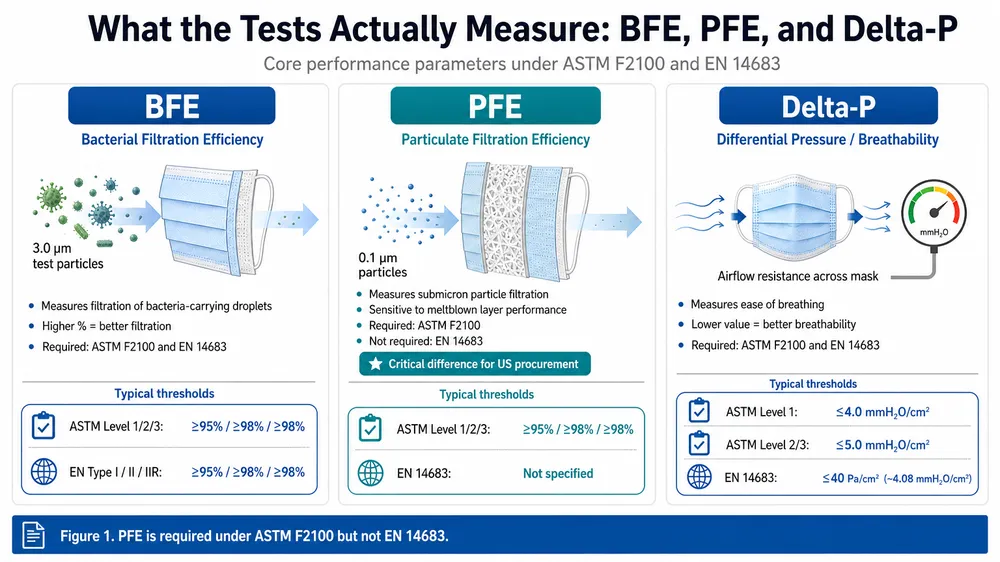
No. BFE, PFE, and Delta-P are properties of the mask body — specifically the meltblown filtration layer — not the attachment method. A mask rated at ASTM F2100 Level 2 (BFE ≥98%) carries that rating regardless of whether it uses ear loops or ties, provided the mask body is identical. Both configurations we produce use the same mask body and the same in-house meltblown layer, so the filtration spec is consistent across attachment styles. If a supplier quotes different filtration numbers for their ear-loop and tie-on SKUs, that's a production consistency problem, not a normal product difference.
What tensile strength should I specify for ear-loop elastic?
The key parameter is elongation recovery — the loop should return to its original tension after repeated donning cycles without permanent deformation. We test incoming elastic lots for both tensile strength and elongation recovery before they enter production as part of our ISO 13485 incoming inspection protocol. Ask your supplier for their incoming inspection spec and test data, not just a verbal assurance. A supplier who can't produce lot-level tensile data for their elastic is not running a controlled incoming inspection process.
Can I order both ear-loop and tie-on configurations in the same shipment?
Yes. We can consolidate both configurations in a single shipment with separate lot documentation for each SKU. The practical consideration is that each configuration has its own MOQ — confirm both before finalizing your order. Mixed shipments are common for distributors supplying both general ward and OR channels from a single purchase order, and the documentation is structured so each SKU clears customs and compliance review independently.
What's the minimum order for tie-on masks?
Tie-on configurations are available with confirmed volume. Send us your estimated monthly requirement and we'll confirm the MOQ and lead time for your specific configuration. Standard ear-loop SKUs start at 50,000 pieces. If you're evaluating tie-on for the first time, we can discuss a sample run before you commit to a full production order.
How do I specify attachment style in an RFQ?
Include: attachment style (ear loop or tie-on), filtration grade (ASTM F2100 Level 1/2/3 or EN 14683 Type I/II/IIR), estimated monthly volume, and target market (US, EU, or other — this determines which certification documentation we prepare). If you have a specific elastic spec, tie material preference, or packaging requirement, include that as well. Send your requirements through our Request Quote page and we'll respond with a spec sheet and unit price within one business day.